
These New Alzheimer’s Drugs Are a Travesty
They cost a ton, have major side effects, and there’s deep skepticism that they even work. So why are we pushing them on patients?

At the Alzheimer’s Association 2022 Walk to End Alzheimer’s on November 05, 2022, in Los Angeles. The group has enthusiastically backed new Alzheimer’s drugs, despite major scientific doubts about their efficacy.
Popular
"swipe left below to view more authors"Swipe →
My father died of dementia. It was a long, slow decline that took almost a decade. Did he have Alzheimer’s disease or some other neurodegenerative condition? I am not sure. As far as I know, there was never a definitive diagnosis. But what my family suffered, particularly what my elderly mother and a series of home health aides endured as they cared for my father, is likely quite recognizable to anyone who has dealt with Alzheimer’s.
The burden of these kinds of diseases is not just the slow loss of someone you love but the enormous amount of support that patients with these conditions require. My mother and father had the foresight to invest in long-term care insurance and had good benefits from their decades as New York City public school teachers. Most families around the United States are not that lucky.
Over the past several years, I have watched the progress of the Alzheimer’s medical field, not as a scientist who works on the disease but as an interested observer. I may not be on the front lines of Alzheimer’s research, but I don’t feel too far away. My interest in Alzheimer’s is personal, but not only because of my father. It is also rooted in the first-person perspective of having lived with HIV for 25 years, and of even more years following the trajectory of research and development for AIDS drugs during my time as an activist and policy wonk with ACT-UP NY and the Treatment Action Group. The desperation and fear many experience with a dreaded disease is not lost on me.
But even though many of us pushed for early access to experimental medicines back then, we always, always led with the data first. We wanted access to new drugs, but also wanted to know what these drugs would do to our bodies—would they help, harm, or do nothing at all? “Access and answers” was our mantra.
I know that what I am about to say might not make me popular in some quarters, but I’m not seeing that same mantra used in the Alzheimer’s field today. In fact, from this one outsider’s perspective, the field is a mess—and so are the drugs.
Let’s start with aducanumab, a drug that targets a protein called β-amyloid (AKA beta-amyloid), which may be associated with the pathogenesis of Alzheimer’s disease. When it went up for approval at the Food and Drug Administration in 2021 (under the brand name Aduhelm), an advisory panel of experts recommended against its authorization, based on the lack of convincing evidence of benefit for the drug. The vote wasn’t close: 10 voted against and one was uncertain. The FDA then decided to approve the drug anyway, against the advice of its own advisers. In the wake of this decision, three members of the advisory committee resigned, with one of them calling the decision a new low for the agency. The whole saga reeked of conflict of interest and backroom deals between the company and FDA officials, leading to exposés in the press and congressional hearings.
This didn’t stop Harry Johns, the millionaire CEO of the major patient advocacy group the Alzheimer’s Association, from praising the approval in gushing terms:
“This approval is a victory for people living with Alzheimer’s and their families. This is the first FDA-approved drug that delays decline due to Alzheimer’s disease. This means individuals may have more time to actively participate in daily life, have sustained independence and hold on to memories longer. We can experience longer—the relationships we hold most dear—our families and friends.”
Johns’s statement is dishonest from start to finish. There is no mention of brain bleeds—a serious side effect of the drug—nor the substantial direct costs of the medicine, the infusions, and all of the diagnostic procedures required with its use. (The Alzheimer’s Association did release an unsigned statement criticizing the drug’s high price, and Aduhelm’s manufacturer eventually cut the price in half—to $28,200 a year.)
It gets worse: When the Centers for Medicare and Medicaid Services refused to cover the drug outside the context of clinical studies, Johns called it “shocking discrimination against everyone with Alzheimer’s disease, especially those who are already disproportionately impacted by this fatal disease, including women, Blacks and Hispanics.” Of course, Alzheimer’s disease clinical trials are shockingly unrepresentative of people of color in the US, with a recent analysis suggesting that close to 95 percent of patients enrolled are white. But leave it to Johns to make claims about equity when it comes to the marketing of a drug that many scientists and experts don’t think does very much at all for anyone and comes with serious adverse events and economic costs, while never noting the fact that just a handful of people of color were enrolled in a study of the medicine. The boosterism here is crass and shameless.
And the circus continues. A new antibody was just given approval by the FDA for the treatment of Alzheimer’s, lecanemab (Leqembi), after the drug showed a benefit against a placebo in slowing cognitive decline. Once again, the Alzheimer’s Association was back to its happy-clappy PR.
“The unquestionably positive data from the clinical studies of Leqembi indicate that thorough removal of beta amyloid from the brain leads to clinical benefit,” said Maria C. Carrillo, PhD, Alzheimer’s Association chief science officer. “This treatment can change the course of Alzheimer’s in a meaningful way for people in the early stages of the disease, allowing more time to participate in daily life and live independently.”
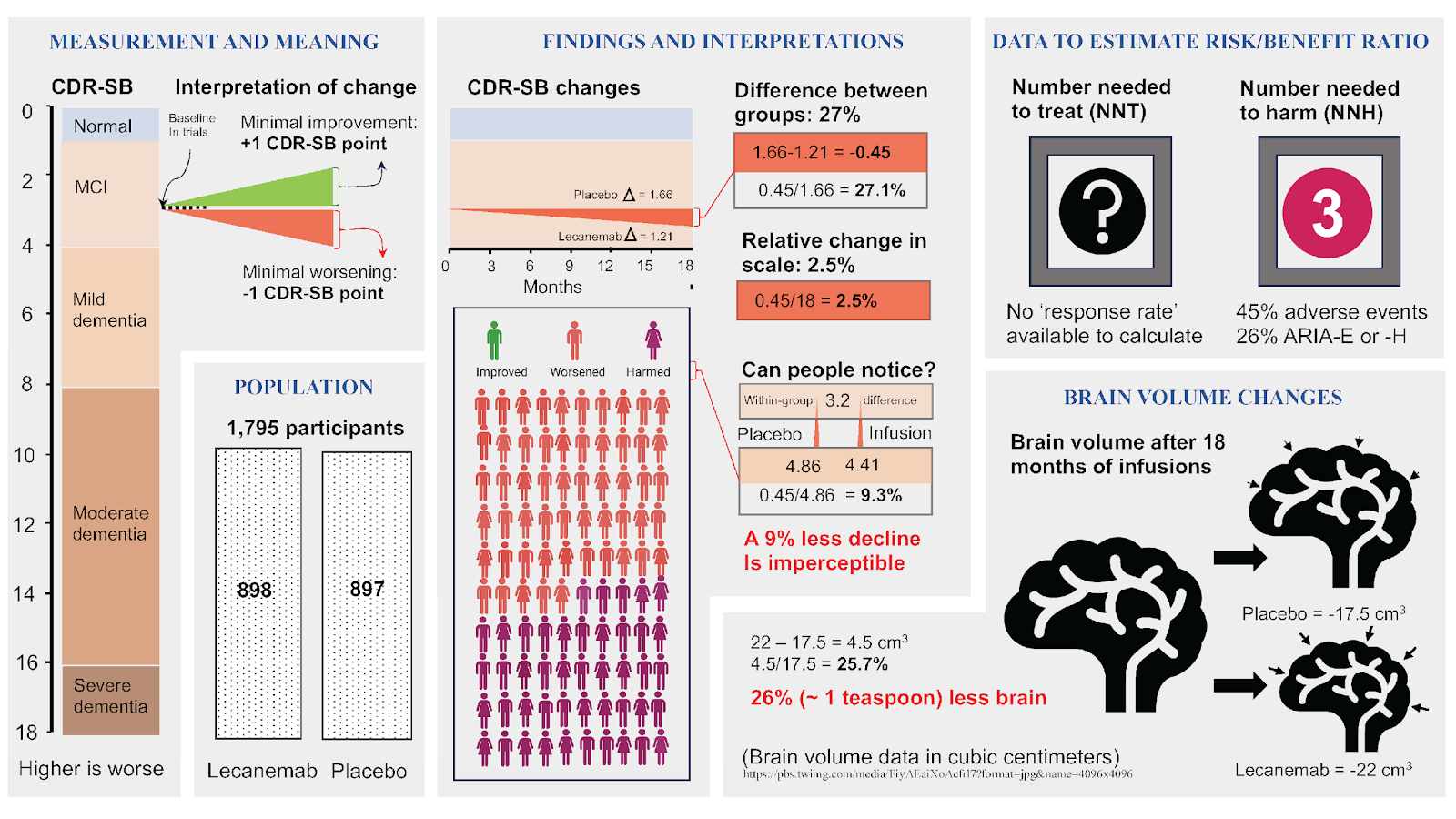
Um. No. In fact, the changes in cognition are minimal. While many of the boosters of the drug—such as the Alzheimer’s Association, some scientists and clinicians, have touted the 27 percent relative difference between the treatment and placebo group in the main study—others are quick to point out that the clinical benefit is unlikely to be meaningful to patients or their families.
Popular
“swipe left below to view more authors”Swipe →
For those who want to dig into the numbers, Alberto Espay at the University of Cinncinati has an infographic that walks through the details of the trial results in patients with mild cognitive impairment. The key take-home? Benefits are likely to be imperceptible and the risk of brain bleeds (ARIA) and other side effects with the drug—like with aducanumab—are substantial.
Meanwhile, the Alzheimer’s Association is rattling on about how the drug “can change the course of Alzheimer’s in a meaningful way for people in the early stages of the disease, allowing more time to participate in daily life and live independently.” This earned the association a stern rebuke from Rita Redberg, the editor in chief of JAMA Internal Medicine, for making claims unsubstantiated by the data.
How deeply, deeply cruel all this is. Here’s another drug, with potentially marginal benefit at best, and well-documented toxicities, which you can’t even take at home (it requires trips to get the medicine infused via IV every two weeks). And lecanemab will cost $26,500 a year alone, with the added costs of diagnostics and follow-up tests estimated to be over $7,000 and with some patients shouldering upwards of $6,000 each year in coinsurance costs as well. All this may add an estimated $2–5 billion annually to Medicare spending in the US. But the Alzheimer’s Association, along with some clinicians, is going full steam ahead with the hype around this drug.
Moreover, the role of β-amyloid and other proteins in the pathogenesis of Alzheimer’s is hotly contested, meaning that it is not certain that it should be used to diagnose patients with the disease in the first place. The prospect of giving otherwise healthy people a diagnosis of disease based on these kinds of controversial biomarkers has tremendous ramifications—for people’s personal lives, their jobs, and their ability to get life insurance or long-term care insurance like my father benefited from.
How many people who might never develop clinical symptoms will have their lives thrown into turmoil from a blood test or a PET scan for amlyoid, even though the science is unclear about the role amlyoid plays? Many proponents of this approach are also suggesting that this will allow us to get to patients earlier, even though many people with amyloid positivity on diagnostic tests may never develop dementia. Given the toxicities associated with the current drugs, their costs and inconvenience, screening a large population of people as candidates for therapy on this basis seems like both clinical and public health folly.
What is also concerning is what the new drugs—like aducanumab and lecanemab—do best: Clear β-amyloid, though with different mechanisms of action. There is thus enormous economic incentive to change the definition of the disease to target the reduction of proteins in the brain, not the clinical manifestations of the disease. It may not help patients, but it will surely enrich Biogen, Eisai, and other drug companies, and the clinical practices that prescribe these drugs.
At the very best, the role of β-amyloid in the etiology of Alzheimer’s disease is subject to debate. Shifting clinical definitions, pushing drugs ahead with little to no perceptible clinical benefit based on the amyloid hypothesis, given the enormous consequences, seems premature, if not just reckless.
But some scientists are even less patient than I am with the current state of affairs. Here is what Derek Lowe, who has worked in the pharmaceutical industry for nearly 35 years, said in Science last year:
I’m not buying it. I am done, and I have been done for several years now. I do not believe that targeting amyloid is going to lead to a useful Alzheimer’s therapy, and watching these trials feels to me like watching someone trying to put out an oil well fire by dumping duffel bags of money onto it from helicopters. Hell, that would probably be cheaper. I don’t know what the answer to Alzheimer’s is, but at this point, as far as I’m concerned, it isn’t amyloid.
But β-amyloid rides on. Funders fund amyloid. Many PhD students study the effects of amyloid, their findings lead to prestigious post-doctoral positions, then senior positions and the circle remains unbroken. If you hear words like “breakthrough” about these drugs, or claims that we’re in a new era of hope for Alzheimer’s disease, it’s because of this self-perpetuating feedback loop inside the field that drives it all forward.
So this is where we’re at, folks. A patient organization running amok, a field that is riven by controversy on basic questions of disease pathogenesis, companies looking to make a killing on drugs with little or no proven clinically meaningful benefit and real harms to patients, and an FDA willing to do their bidding. This is a race to the bottom, incentivizing the worst behavior of everyone involved. Those who have succumbed to neurodegenerative conditions such as Alzheimer’s, like my father, and those now living with the disease all deserve better than this.

